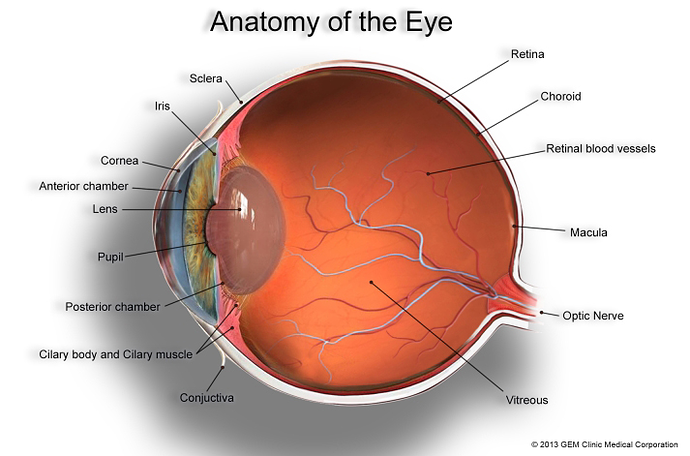
Ok. Eye injuries... phew. I finally am circling back. A brief disclaimer, eyes are incredibly complicated and this is not my area of expertise, but I can give you a few basic principles to work off. For reference to the parts of the eye I'm going to talk about, I've attached this image:
Biggest point: depth matters.
Lacerations to the eyelids, conjunctiva, sclera, and cornea will heal without interventions, causing no permanent damage. These are the most common types of lacerations when dealing with slashing injuries, because the brow and cheek bones create a concave space for the eye which protects it from slashing motions. Damage the lens can be more severe, but lens replacement (often called cataract surgery) is a 15 minute procedure that easily can fix lactations to the lens.
If the damage is deeper than the sclera, puncturing the vitreous, then removing the eye is often necessary, depending on the width of the laceration. However, we can replace eyes pretty easily, so you don't need to have an empty socket for life and can regain full vision. If we don't replace the eye, we can surgically suture the retina closed and leave the native eye in place. You'll be blind (not true blindness, because you will still see light) and often won't have an iris (just a really big pupil), but you don't have to remove eye all the time, because as long as the blood vessels are intact, it's not going to hurt you. I can easily see magical healing being able to replace your eye with someone else's eye or repairing a damaged retina.
Any deeper than the vitreous and you risk damaging the macula and most horrid optic nerve. Damage to the macula will of course cause blindness, but again can be treated with eye replacement surgery. Optic nerve damage means irreversible blindness. Whether we remove the eye or not sort of just depends on how clean the cut was, how thin it was, and how much tissue of the native eye is salvageable. For cosmetic reasons it is always preferable to keep the eye in place if we can, but if we do remove it (because it's just too cut up to salvage) we won't do a transplant, because there is no point with optic nerve damage. However, you can have a glass eye which removes the need for an eye patch.
And speaking of eye patches: they are used to keep the eye protected and hydrated during the healing process. Often we use eye patches if there is damage to the eyelids or muscles of the eye, because we need to keep the eye closed while those areas heal.
A note about injuries to the muscles of the eye, those will obviously affect vision, but can heal spontaneously or through surgery as well. Or you might just have a lazy eye.
Finally, what causes white eyes? Not blindness. The classic sequence where the eye clouds over in seconds after a blinding injury is just wrong. White in the lens of the eye is caused by protein accumulation, called a cataract. Cataracts are more common in blind individuals, which is why we often associate them with blindness, but not all blind individuals will necessarily develop cataracts. There are other conditions that can cause cloudy appearance in the eye (scar tissue as seen in the retinal repair image I attached above), but the most common reason is cataracts.