
Gross. Good luck! Taking this info into account, as an added side note to your question about bleeding, if your character is chopping off body parts after death, those new wounds won't bleed.
1 month later

3 months later
Hey authors! I’m back to talk about more medical tropes that bother me, because it’s about the only thing that ever does and I can.
This time I’m giving you three tips for how to write realistic hospital scenes.
Hospitals don’t have a smell. At least we try really hard not to. We use odorless cleaners, lotions, air fresheners, and soaps. I’ve heard some authors describe hospitals as having an antiseptic smell, but even our hand sanitizers don’t have that alcohol smell that commercial brands do and bleach is very rarely used, so the only smells in hospitals come from patients and those are usually horrible. Trying to maintain odorlessness (not even clean smelling, but truly no odor) is intentional as many people are sensitive to smells.
Heart monitors don’t beep continuously with the rhythm of a patient’s heart. Like, they can, but it’s super annoying and the default settings on monitors is silence. Believe it or not, nurses actually try to minimize noise and alarms in the hospital. Sometimes it’s hard to do, but there is almost always someone around to address an alarm and silence it. Every alarm has a purpose and requires nurse attention. In fact, the only thing I hate more than alarms are patients who silence their own alarms.
 Do as I say, not as I do.
Do as I say, not as I do. 
Last, but most importantly, nurses never want to be hit on while at work. Ever. It doesn’t matter how cute the patient is, hitting on a nurse is always inappropriate and so uncomfortable. Does it happen? Yes. Absolutely. So much so that it is extremely triggering for most nurses. I’ve seen a lot of comics out there lately about nurse-patient relationships. I think this can be done alright (like in the comic Nurse’s Station), but most of the time it’s not (like in Heroic, which btw I love, but can’t stand how the propagandist is constantly flirting with his clearly uninterested nurse.) On a related note, nurses don’t hit on patients. I’ve literally never seen or heard of this. There are horror stories of medical professionals sexually assaulting patients, because, hey, it’s 2022, and there are psychos in every profession, but legitimate flirting? Nope. I have taken care of thousands of people and seen just as many boobs and penises, and I’m bisexual (so I’m not particularly picky under normal circumstances) and I have literally never been attracted to a patient nor have I heard any of my colleagues commenting on a patient’s appearance. It is one of my number one pet peeves in media when I see a group of giggling female nurses oogling over the male lead’s abs. No. Nope. No. Gross. That it so unprofessional and just wrong. It is my personal opinion that no one should objectify someone they are authority and stewardship over.
So there you have it! My thoughts on common hospital tropes!  ️
️
Do you still review comics or novels for medical accuracy? I have one medical subplot and although not a turning point of the story, it's still kinda relevant for the characters involved. The epidemic is chickenpox and the world is reliant on magic so their medical isn't that advanced. The cure they came up with is chamomile. I'll put the link here, if you no longer do this favor, then please just disregard this comment
The topic is brought up in this chapter:
The cure is brought up in this chapter:
No need to read most of the in between chapters
Again, if you're still entertaining questions... (I came across this thread since someone bumped it, and I plan on reading everything as I go on, so I don't know yet if you already closed the questions since another person bumped it)
My character has reincarnated in a completely different world with magic and whatnot but has memories of her past life (Earth). My character remembers the reason why she died. The character is also made aware of how she reincarnated in this new world right off the bat so she was able to "process" things and calm herself, being able to remember bits and pieces of her past life (with the help of someone close to her in her past life). But she doesn't remember all of it and some of her "memories" are just things that she thinks happened, but not really. There are memories that she thinks happened, but not really. There are important/significant things that she forgot but is able to remember some insignifacant things from her past life.
Do you think it's possible or understandable that the character is experiencing/feeling this type of "jumbled" memory? Is it reasonable that she forgets her own (past life) mother only after eight years of living a new life? Or is that too short of a span of time to forget what your own mother looks like?
I absolutely am still entertaining questions! I always love to help out authors. 🥰 Give me until tonight and I’ll have a reply to both your questions up.
How many questions do you entertain per person? just curious...  <--- it's supposed to be an awkward smile....
<--- it's supposed to be an awkward smile....
Goood this is sooo helpful! thanks for this thread!
Do you have any info on Port-wine stain (aka nevus flammeus)?
I have a character who was born with fair skin but developed reddish-purple patches on his skin as he got older. I am not sure if I should label my character as having port-wine stain or just make up a fake condition that is similar to it (my comic is a fantasy).
Sure! This is an easy one.
Nevus Flammeus is a congenital condition, so your character would be born with it. It does not develop as you age, but can become more prominent or expand with age.
However, there are other conditions which can cause red, purple, and brown patches. Where those spots appear, what they look like, how large they are, and what color they are will determine what they are called.
Granuloma annulare is probably the closest thing I can find to portwine stains that occurs in adulthood. They are commonly found on the ankles or hands and are painless, red/purple patches that develop over time, typically in adults.
Other Painless Spots:
Liver spots are common on the arms and abdomen while melasma are found on the face. Both are painless, benign (meaning not life threatening) conditions. Purpura can cause purple-red spots and are common in old age. In younger characters (under 65) it could be an indication of an underlying bleeding disorder. Scleroderma are very small purple-red spots that sometimes look like an exploding starburst. Morphea are light brown, sometimes large spots that can cover the face, neck, and torso. Keloids are purple-red raised scar tissue that can expand from an injury to cover a ton of body surface area. So if your character was cut by a blade or knife he might have keloid formation over those spots, extending into massive purple-red lesions. Spider angioma can be small purple spots which look like spiderwebs.
Everything else which is not infectious related will be itchy or painful.
Annoying/Itchy Chronic Discoloration Lesions:
Nummular eczema causes red, sometimes purple patches on the skin, but are extremely itchy and lesions will move over time. Uritcaria pigmentosa lesions are sometimes brownish red, but this is more commonly found in children and usually clears by adulthood (although it can stick around). Psoriasis causes purple-red elevated plaques of dry skin (often flaky and white) commonly over the knees and elbows, but can happen anywhere (although generally not the face) and are extremely uncomfortable (but is a chronic condition that people just live with and often don't get treated ever).
Let me know if any of these conditions peak your interest and you would like any more information!
For a full description of real-life amnesia please refer to my second post in this thread.
Advise for you specifically: Everything you described sounds like magic, so it can work anyway that you want it to work! Red-flags for "this is not real-life amnesia, but magic amnesia" are discussed below:
Confusion and missing sporadic memories is common in short-term amnesia related to underlying infections or diseases, but does not occur in long-term memory loss conditions. Typically amnesia will affect the newest memories first and the work backwards chronologically in large chunks rather than sporadic, patchy memory loss.
Confabulation of memories is something everyone does all the time, but it's not really associated with amnesia nor are the confabulations typically implausible. Confabulation typically occurs during high emotion time periods, such as death, weddings, stress, life changes, or really anything "big". Like, you may think that your brother attended your wedding, when he really didn't. Or you may think that your mother was being aggressive and defensive after the death of your father, when she really wasn't. Stuff like that. People with memory loss don't "fill in" the details with full-on hallucinations (like you aren't going to think you had a brother that you never had).
Typically significant things are what we remember the most. Insignificant details are often lost, because they are not associated with strong emotions. People nearly always remember their family members, but will probably forget who the president was when they were 12 or the layout of their house when they were 20.
Nope, unless it's magic! So it's honestly whatever you want.
Forgetting visual memories is much easier than categorical memories. Absolutely she might not remember the details of her mother's face, but she will probably remember her name and what her personality was like and what she did for work. She also would probably recognize her mother if she ever saw her again. Recognition sticks around for a VERY long time.
Conclusion: A lot of this sounds like magical amnesia, which is A-ok, because it was caused by her dying and being reincarnated. That bothers me WAY less than magical amnesia caused by a head injury. Head injuries are real things that cause real amnesia states. Reincarnation not so much, so the rules can be anything you wants.
Chickenpox
For the most part your description of chickenpox is spot on. It is a highly contagious viral infection with a rash characterized by itchy, blistering red spots. It does usually resolve within 2 weeks if not sooner.
A few points:
Isolation can be as simple as wearing gloves, gown, and mask and sanitizing surfaces with boiling water or bleach. It's not airborne, so they don't actually need to be isolated to the point where no one can see them. A simple face covering and barriers between your skin and the infected person's is sufficient to prevent the illness.
Itching can be prevented with mittens. This is a great idea and much better than encasing them in a blanket. That's just going to make their fever worse and dehydrate them. Speaking of which:
Hydration: Absolutely the more water the better.
Rash: Viral infections do not cause pus formation (particularly not yellow-green pus). A secondary bacterial infection of a varicella rash could cause white (barely yellow) pus to drain from the blisters but this is pretty rare. It's more likely if the patient is colonized with staph and scratching, so points for accuracy there. Bacterial infections are treated completely differently and are typically more deadly and not self-limiting (like most viral infections).
Seasonality: Viral infections have hardly anything to do with the weather. This is a common misconception, so you can keep the part where she says, "more likely to get it when it's really hot", but just know, it's not true. Extreme heat actually deactivates most viruses, including the varicella virus, which is why summertime is when you are least likely to contract chickenpox. Peak times for chickenpox are in the winter and spring when people are gathering indoors and traveling more (think Christmas, spring break, etc.). This is related to population behaviors during those months, not the weather.
Homeopathic Treatment: There is not evidence to suggest ingesting chamomile will decrease the infectious period of varicella infections. Chickenpox is self-limiting, meaning it does not require any specific treatment, however there are several herbs I suggest that may facilitate recovery. First are the standard immune boosting herbs: elderberry, vitamin C, and zinc. Second are the antiviral herbs, specifically those that have been studied in varicella: licorice and lemon balm leaf can both be made into teas and administered every few hours. Both can also be made into topical salves which can ease pain and reduce severity. Both of these herbs have good evidence surrounding their antiviral properties, including protein denaturing and mRNA replication disruption. Honey applied directly to the skin also has antiviral properties and can help sooth itching.
Overall, great job. The only things I would change are the pus (unless you really want to go the secondary bacterial route), chamomile to some other herb I mentioned, and maybe the part about hot weather increasing infectiousness (but this isn't something most people know, so eh.)
Wow- I just discovered this thread and I'm amazed by how thorough and well-thought out your responses are and that you've kept up with it for so long. Thank you for taking the time to help others improve their stories! This is an absolute blessing for us writers who don't know the first thing about anything medical-related (i.e. me lol) 
I have two significant and spoilery scenes planned for my story that will cause severe injuries for some characters, so I'll avoid mentioning names/genders/context. I've done some research and consulted a nurse friend, but haven't decided exactly how I'll write them yet nor worked out a good, non-hokey balance between the realistic consequences and the life-saving magic of an ancient fantasy kingdom setting. Any advice?
One scene has a fighter break a couple ribs, a few fingers, and lose an eye when it's slashed by a blade, then spends a period recovering and learning to adjust. After those injuries, what would recovery look like and how long would it be before the character could fight/be active again? Does a slashed eye always need to be removed, leaving an empty socket? (I've seen several half-blind characters in fiction with slashed eyes that simply turn cloudy and blind and always wondered how realistic that is)
The other event has a character go into a coma for several months (edit for context: due to a head injury, is also beaten and stabbed multiple times). Considering the fact that it's so long-term and involves a developing young person, I know a full recovery and regaining their pre-coma mobility would be impossible in reality, so I intend to apply magical healing generously here. Nonetheless: What would the character's care while comatose look like? What would recovery look like?
Though magical healing is magical and the fact that my characters aren't human gives me leeway, I don't want this to negate the impact of their injuries. I'd like these scenes to have weight, impact, and consequences, with time devoted to healing and adapting to long-term/permanent effects... but also need my characters to regain enough functionality to eventually participate in the action again.
 You're so sweet.
You're so sweet.As long as the fractures to the ribs and fingers are all simple (meaning they don't puncture the skin or any internal organs) they will both heal on their own without any intervention within 6 weeks. They can definitely fight after that, no problems. You can brace the fingers, but it's not really necessary. Ribs we do literally nothing for, except advice them to not lift anything heavy and brace with a pillow if they cough or vomit. I'm gonna skip the eye injury bit for right now and circle back around later.
Phew, ok, so comas don't typically happen with head injuries or being beaten or stabbed. I've talked about this before in this thread (somewhere?), but lose of consciousness is either a sign of an acute illness (infectious, liver failure, some rare autoimmune stuff) or increased intercranial pressure (ICP). Increased ICP does occur after traumatic brain injuries (TBI) if you are having a hemorrhagic stroke, i.e. a bleed inside the brain. This needs surgical intervention (usually removing a part of the skull to allow the brain to expand outside the closed box and drain placement to remove blood.) I suppose magical healing could help the body reabsorb blood faster and stop bleeding by repairing the damaged vasculature, but that would basically make the person wake up immediately. Often after surgery we will keep patient's sedated using medications while we treat other injuries or wait for ICP to go down (using a drain). Sometimes medically sedated patients can remain comatose for several days (rarely weeks) after we stop the medication, but this only really happens if we are using those medications for a long time (weeks to months). If you hear of someone "waking up" from a coma after a couple of months, this is because the physicians were giving that person sedating medication at some point. Bottom line, if a person is not on sedating medications and is 24 hours post TBI and they aren't waking up, they never will.
On the flip side, if a person is being medically sedated for months and regains consciousness, recovery for mobility is often fantastic. Hemorrhagic strokes rarely affect motor centers of the brain, more often targeting speech centers and decision making centers (frontal lobe of the brain: the part that makes you you). If the person is affected in the motor complex, physical and speech therapy in the months immediately following the brain injury can greatly improve outcomes. The brain is stupid plastic (adaptive) and injuring it is nothing like injuring the spinal cord. The reason TBI's are so scary, honestly, is because a lot of people just don't survive, don't ever "wake up", or have permanent personality changes afterwards (poor decision making skills and impulse control). Of course, lots of people have persistent weakness and balance issues that can plague them for life after a TBI, but way more fully recover motor function, particularly if they go to physical therapy religiously.
Thank you for the in-depth responses! This is super helpful and gives me a lot of good food for thought! :]
Pretty sure I've covered this in the thread.... hang on... oh wow, I guess I haven't. That surprises me. Ok. Let's talk Care of Unconscious/Immobile Patients:
- ABCs: Airway, breathing, and circulation are huge priorities in the care of unconscious patients. Almost universally, patients who are unconscious will be intubated and ventilated. This means a tube is inserted through the mouth (rarely the nose, sometimes cut straight into the throat although that's called a tracheostomy) into the trachea (airway). This is because unconscious patients are at risk for their airway collapsing and cutting off breathing. If they have any kind of respiratory problems (like pneumonia which is stupid common in unconscious patients) they also need to be ventilated to support their breathing. And of course, even if they are breathing fine and their airway is alright, they might not be circulating enough oxygen which is another reason we may mechanically ventilate them.
- Skin: This is another zinger. Have you ever sat on your butt for too long and felt pain? That is because the arteries that are supplying blood to your skin are compressed for a long period of time, denying the skin of oxygen. If this happens for too long, it can cause a pressure ulcer (content warning for picture) to form at pressure points (most commonly over the coccyx and heels). In order to prevent pressure ulcers, nurses or nurse aids turn unconscious patients ever two hours. Some hospitals have specialty beds that can rotate patients or redistribute weight using variable air pockets, but people still need to be manually turned. We can also use pressure ulcer prevention dressings, which are these big pink form patches that go other the heels or butt and help redistribute weight over bony prominences. Again, you still need to turn patients to prevent pressure ulcers even with devices helping you. Turning them basically just involves tucking a pillow under their left or right hip or removing the pillow to lie them completely flat (three positions).
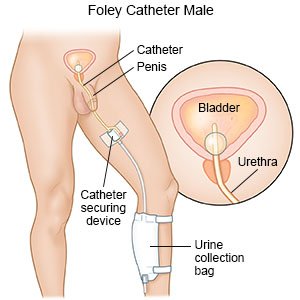
- Urination: Of course you still need to pee when you're unconscious. We frequently use urinary catheters to catch urine and hang the collection back below the patient (using gravity to drain) on one of the bed's hooks as seen here. For people who are unconscious for more than a couple weeks we just use absorbent pads or diapers which we check whenever we turn them, because urinary catheters can actually cause infections (UTIs).
-
Defecation: Immobile patients often have constipation. Walking helps stimulate the bowels, so if you don't move, you often get constipated. Also, the drugs we use to sedate people cause constipation. So nearly all unconscious patients will receive stool softeners (like senna) every twelve hours. And of course, someone has to clean them up.
- Eating: Not necessary unless you are unconscious for more than 3-4 days. Seriously, people worry all the time about us starving their family members, but we typically don't start them on a diet until day 4 or 5. We use kangaroo pumps to deliver liquid goodness (totally kidding it smells and taste God awful) through a tube that is inserted into the mouth or nose and passed into the stomach or small intestines.
- Hydration: Sedated patients are more often than not over hydrated. This is another thing families worry about, that they really shouldn't. We give people so much medicine and they often retain water. However, we check sodium levels in the blood every twelve hours anyways, which will give us warning if they are dehydrated. Also, if they have a urinary catheter, we expect them to produce at least 30mL of urine every hour. If they are doing that, they are hydrated. If we do need to give water, we can do it through an IV (0.9% sodium chloride sterile water, often just called saline) or through a feeding tube (tap water is just fine).
- Bed Baths: at least once a day, sometimes more often if they are real poopy. This just involves using wet wipes (think like baby wipes) to clean the skin.
- Blood work: Typically we will do blood work on conscious patients every twelve hours for... lots of reasons. Hydration, electrolyte balance, blood oxygenation, kidney function, anemia, and just too much to go into, but yeah, unless a patient is stupid stable (meaning there has been no change in their treatment plan or blood work for 3 or more days) we will do blood work. This might involve sticking them with a butterfly needle or drawing blood from a catheter (IV).
- Contractures: Immobility causes the muscles to contract and stiffen. We place patients in neutral positions to prevent this a much as possible, but if someone is truly immobile for months, they will need someone to move their feet, arms, and legs through range of motion exercises to prevent muscle spasticity. For a good image of what contractures looks like, just think about someone with a spinal cord injury. Basically everything flexes (fingers curl, biceps flex, wrists curl, knees bend, feet drop).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/GettyImages-453885149-1cee51d638db4f93ae69933d389bffc6.jpg){kind=link}
Hm... maybe that's it? I'm sure I'll think of more stuff later, but those are the big things.