
Ah!
Thank you very much for your response and explaining 
I appreciate it very much.
The driver was actually just holding the steering wheel and shooting at chasers by her gun
The one beside her, was sitting on her knees, because she was shooting with arrows (archery).
What can happen to the front seaters now?
Can the driver's hand get cut or anything?
Can the archery one get a knee fracture or something?
Backseaters were bent down, what can happen to the back seaters?
Thank you again!
I admit I haven't read everything and mostly skimmed the answers to see if you had already answered my question, but didn't see it. If I am wrong please feel free to let me know it's been answered already and i can more thoroughly look through what is already here. I'm also not sure if this info is anything you would know, but figured I'd ask!
Do you know what happens after someone dies? Some specific questions I'm curious about: how long does a hospital keep a body before it is taken out. What type of storage process happens? what employees have access to the dead bodies? Do dead bodies bleed much afterward? Does everyone get autopsies or is that a criminal case only thing? how does organ donating work? But anything else you can share about it would also be appreciated.
Thank you so much for this thread!
A lot of medical stuff I do is from personal experience, but I wanted to ask specifically about brain damage. Allie hasn't been in the comic much yet, but here's the link if you're interested:
So Allie has brain and spinal nerve damage from an electrical injury. She's had a lot of years to recover. Symptoms wise:
-Most movement takes her conscious effort, so her movement and speech is quite jerky and slow, including her speech. She uses arm crutches for balance.
-She has weak grip strength and trouble bending over
-She has a service dog mostly trained to carry objects
-She doesn't have much in the way of impulse or mood problems, though she did early in treatment.
-Chronic pain issues
-She does regular occupational therapy and checkups
Do any of these feel off? Is there something glaringly missing?
Thank you!
I have a follow up question, if you're still answering them!
Re: weaning patients off of sedation, what does that look like? I assume the drugs would be administered via IV, but I don't really know how that works/gets turned on and off, and this info has been harder to google than I had expected.
Thanks again for all of the great information!
Sorry for being MIA for several days.
Ok... I will walk through mechanism of action for the injuries one by one. (These are just suggested injuries based on my own imagination of what the accident could look like. You can certainly change things based on what the characters are doing at the time of the accident.)
Front seat driver: I imagine that if their arm is out of the window at the time they run into the pole, their forward moment would continue pushing their arm forward and their humerus would hit the side of the window. Dropping the gun seems likely at the very least, as well as a transverse fracture of the humerus. If you want to make the break minor, it could be just a hairline fracture, not requiring casting. This type of fracture does not go all the way through the bone and results in pain, bruising, and swelling. It is possible that the driver has a minor abrasion on their arm, but this wouldn't bleed too much, because it would be fairly superficial. Obviously, the driver's head is also turned to the side, because they aren't looking. When the airbags deploy, their neck will probably be further kinked to the side, resulting in some neck pain or stiffness for the next two or three weeks. That's about it for the driver.
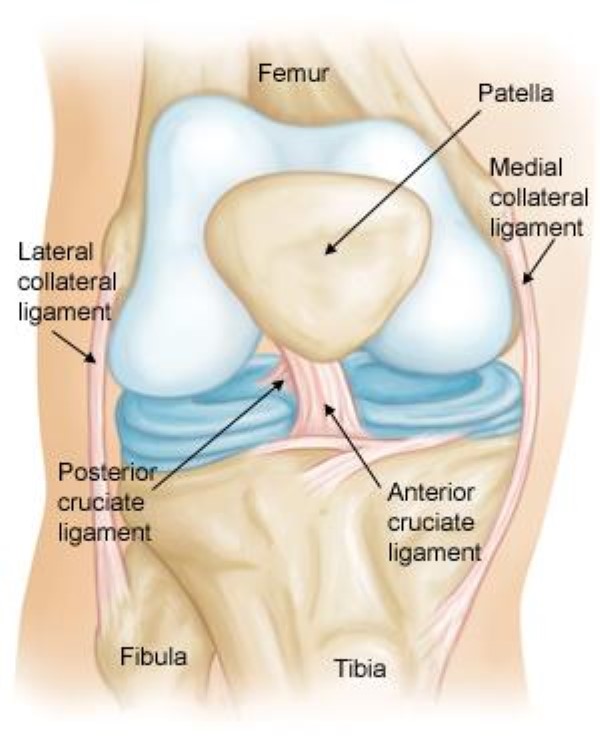
Front seat passenger: I'm trying to envision how she is shooting arrows out of a window and I just can't without her leaning all the way out of the window. Does this mean they are riding in a convertible? She is kneeling facing the back of the car? Wearing a seatbelt or not? I'm gonna assume that maybe she is just leaning REALLY far out the window with her bow in hand. In this case... she probably would be thrown from the car and likely have permeant and very severe injuries unless they were moving really slow. Let's assume she isn't thrown by some miracle... Her abdomen would hit the front side of the window, just like the driver's arm. This could result in some serious internal damage or (if she has lots of nice padding there) just some minor swelling and bruising. She actually might get a little constipated for the next few days as the bowels can shut down after trauma to them. Be sure she takes some stool softeners to prevent an obstruction!! HAHA. As far as a knee injury? I don't think that is likely. Unless her knees hit against something hard, which I just can't wrap my head around seeing. But I'm not the most visual person ever, so I'm sure you could make it work if you really wanted to. If the knee is hit straight on, it could result in a comminuted fracture to the patella or a tibial plateau compression fracture, but those are pretty rare. More common knee injuries are due to twisting or tearing of the ligaments or meniscus. They may have a radial tear of the medial (inner) meniscus of the left knee or lateral (out) meniscus of the right knee if they are kneeling facing the passenger side door. Similarly, the medial collateral ligament of the left knee could tear or the lateral collateral ligament of the right knee. If the passenger is facing forward, the tear would occur on the posterior cruciate ligament. If they are facing backwards: the anterior cruciate ligament. These sorts of injuries heal on their own, but can cause chronic pain for a person's entire life without physical therapy. Lifelong implications of knee injury include osteoarthritis later in life. Short term implications include pain, swelling, destabilization of the joint (leading to difficulty walking and further injury if not braced), and "popping" or "grinding" sounds or sensations.
Back seat passengers: Don't bend down. This can actually cause really bad neck injuries if they hit their heads on the seats in front of them as the head is hyperflexed. At the very least, they will probably have neck stiffness and possibly a concussion. It all depends upon speed of the crash. Anything above 30 mph could lead to permanent brain or neck injury if a passenger is bending down like that. Alternatively, nothing could happen. Honestly, it wouldn't bother me at all if I read your story and the back seat passengers walked away scotch free.
Hope this helps!!!
GREAT QUESTIONS!!!! I know TONS about this! I deal with people dying almost every time I work, so I'm pretty familiar with this process. Of course the process is different if you die outside the hospital, but that's doesn't sound like what you are looking for so here we go!!!
After Death Care
1. As soon as my patient dies, I, the nurse, contacts the family. Often that means just walking into the room and telling them their family member's heart has stopped. I express my sympathies and offer them food, drink, tissues, etc. I encourage them to stay with their family member to take their time to grieve.
2. Then I contact several people very quickly. First is the doctor. If the death was unexpected, often the doctor is already there. However, often times we know they are about to die and are just waiting. In either case, the doctor needs to be present to pronounce time of death. The doctor will also ask the family if they want an autopsy. Autopsy is not available if the patient died due to a communicable disease (like COVID) and most family members do not want autopsies in my experience. Autopsies are only required by law if homicide is suspected or if the body was altered by a fire.
3. Second, I contact the chaplain who coordinates with the family's chosen mortuary. In some hospitals this role is fulfilled by a palliative care team, hospice team, or social worker instead of a chaplain. The chaplain talks to the family, providing comfort and talking them through the next steps. This includes choosing a mortuary if they haven't already. Most hospitals allow families to stay in the room with the family member for up to two hours before we need to take the body down to the morgue, but some hospitals allow longer or less or don't have a set policy.
4. Third, I contact donor services. Based on the information I give donor services (cause of death, age, chronic diseases) they will determine if the patient is eligible for organ or tissue donation. Most people are not eligible for organ donation, but are for tissue donation. Eye donation is also pretty common. If the patient is eligible a representative from donor services will come to speak to the next of kin about donation. Nurses, doctors, and other hospital staff NEVER do this and I'm super glad that there is a policy against speaking about donation to family members at my hospital. I don't like talking about it personally.
5. I may or may not do a little bit of postmortem care just to make the person appear to be sleeping for the family. This includes removing a breathing tube if it is place, closing their mouth, turning off monitors, and removing obstructing machines (like IV pumps, central monitoring devices, or ventilators). As a side note, I don't know why every TV show has heart monitors making that annoying beeping sound continuously, but they don't beep continuously. Any noise that comes from monitors is always an alarm to notify the nurse that something needs attention. I will very quickly silence those alarms while I assess the situation, because they are VERY annoying. The alarm that signals cardiac death or asystole is not a straight tone like seen in movies. It is a loud beeping alarming sound and I pretty much turn that off as soon as I walk in the room after a patient dies. (That's assuming it is an expected death. If it unexpected and we were doing CPR, someone is always around silencing the alarms. Codes are actually pretty quiet, because we just can't think with an alarm blaring. We all know the person's heart has stopped, we don't need an alarm telling us that. haha.)
6. After the family leaves (usually after an hour or two), I with some of my nurse friends will prepare the body to be taken to the morgue. (In some hospitals during daytime hours the mortuary will actually come to pick up the patient directly from their room, assuming they are not a candidate for organ donation or autopsy or the family refused both.) I clean the body with wipes, remove all IV lines, tubes, monitors, etc., and remove all clothes and personal items (like rings which can become stuck on the patient if left too long after death due to swelling and rigor mortis). I actually try to send jewelry with the family before they leave, but otherwise these personal items just go with them to the morgue and then to the mortuary. For example, if a patient doesn't have any known family or they can't come for some reason, a person's phone, rings, clothing, and shoes will just travel with them until they reach the mortuary. Wallets we keep on the unit in a lock box until a family member can come pick them up, because they usually contain personal information which is a liability if lost. We label everything with a patient sticker including the patient! They get a tag on their chest, around their toe, and keep their patient arm band on their wrist. Then I put them in a white body bag (double bag for communicable diseases) and call the morgue to come pick them up.
7. The morgue transports them from their room on a metal gurney with a sheet covering the body bag (don't ask me why, because it does nothing) straight to the mortuary. No stops, no chats with coworkers, no chances for someone to just "switch the body". Most of the time, they are transporting the body through the "core" of the hospital instead of the "patient facing" parts. This is a design of most newer hospitals in which the center of the hospital is basically the medical team's workspace that is never seen by patients except during transport and not at all by family members. The core is locked by badge-key access and contains staff and patient transport elevators, medication rooms, break rooms, equipment rooms, tube systems (for sending blood and medications to lab and pharmacy) and rounding rooms (for all sorts of meetings). All these rooms are locked by keycard access and some hospitals even lock their internal elevator systems to avoid patients and family members from using them. This includes the morgue which is locked by keycard. The only people who have access to the morgue are transporters, morticians, medical examiners, nurses, physicians, and cleaners and maintenance workers specifically assigned to care for that area of the hospital. Sorry for all the security talk if that's not relevant to your story, but I hope you find it interesting either way! What I'm trying to say is, someone could steal a badge and access the core of the hospital, but then find out they can't access the morgue.
8. Storage fridges are a thing! Morticians and medical examiners are the only people authorized to access the body after it reach the morgue and some modern hospitals have individual locks on the fridges to keep unauthorized people out. Medical examiners will perform autopsies and donation services will harvest tissues and organs in the morgue. Is is all done pretty quickly, usually within the first 24 hours. I've seen eye harvesting before and it literally takes 15 minutes. Super fast. Other organs can take longer and (of course) some organs can only be harvested immediately before or after death (such as the heart). That process is a bit more complex and super rare. Autopsies are also usually pretty fast (1-2 hours) and done all in one sitting (so the body is never just lying out unattended in the morgue.) Results from an autopsy (final reports and lab work) can take days to weeks however. But we don't keep the body during that time, we just contact the family once the report is available. Typically families want to claim the body as soon as possible after death, so we don't keep bodies longer than a day most of the time. How long a hospital we keep an unclaimed body varies from state to state and country to country, but most of the time not longer than a week and my hospital is only 48 hours. Unclaimed bodies are offered to the state for research and then cremated or buried (depending upon local laws) if rejected.
9. Whether the body is claimed by the family's chosen mortuary or given to the county mortuary after being left unclaimed, the mortuary will pick up the body from the hospital and transport it back to their facilities. Some mortuaries are funeral homes with very low security, while others are more sophisticated. Regardless, they perform the embalming and cremating process.
10. Funerals typically take place about a week after death and I think we all know how those work. 
Fluids after death
The only question I think I didn't cover was how much dead bodies bleed: the answer is they don't. Pretty much as soon as the heart stops beating you stop bleeding unless there is a really big open wound through with the blood is "falling". Even then, it sort of depends upon gravity and the site of the wound. For example, if someone had a gunshot wound through their abdomen, that wound would pretty much stop bleeding within a few minutes after the heart stopped beating, but when I remove arterial lines from a patient's wrist (which are super special IV's that monitor a patient's blood pressure continuously), those can bleed even an hour or two after death, because it is basically a hole in the patient's blood vessel (artery). If there are no open wounds, the patient won't bleed, and if their are open wounds, the blood flow will be very slow and easy to stop after death, because their is nothing moving the blood.
More commonly, after death, people will release their stomach, bowel, and urinary contents. All those sphincters (esophageal, anal, and urinary sphincter) relax, so patient will pee, poop, and regurgitate. Although, the vomiting thing I will mostly only notice when I turn the patient onto their side in order to clean them or put them in a body bag. I always put an absorbent pad underneath their face the first time I move them to catch any stomach contents that may spill out of their mouth. Sorry if that's a disturbing imaging.  Depending on what caused the death, patients might also have a LOT of edema (which is basically water trapped inside their tissues, think when your feet swell up after sitting for too long). If the edema is bad enough, it can actually leak through the skin after death and make the patient's skin very thin and fragile (like wet phyllo dough). In that case, the outer most layer of skin can actually peel off and release all that trapped water. This only happens in very advanced chronic diseases like alcoholic cirrhosis (don't drink everyday kids!).
Depending on what caused the death, patients might also have a LOT of edema (which is basically water trapped inside their tissues, think when your feet swell up after sitting for too long). If the edema is bad enough, it can actually leak through the skin after death and make the patient's skin very thin and fragile (like wet phyllo dough). In that case, the outer most layer of skin can actually peel off and release all that trapped water. This only happens in very advanced chronic diseases like alcoholic cirrhosis (don't drink everyday kids!).
If you have anymore questions or something was unclear, let me know! Happy writing!
Great question! I've answered this in part before here:
Other notes that may be helpful:
Sedation is given through an IV continuously. This means we use an IV pump1 to give the medication. Propofol is my favorite, because it has a very short duration of action. Usually within 10 minutes of me turning off the propofol a patient will start to wake up. Fentanyl, versed, and diazepam can take an hour to even days (depending on how long a patient has been on the medication) to clear the system. The nurse will slowly turn down sedation every hour or so until the patient is at the minimum dose. As long as the patient is calm and cooperative, we will continue to go down until the medication is completely turned off. The goal of any sedation is to give the patient the minimum they need in order to be calm and comfortable. I've seen patients on a ventilator for WEEKS without any sedation at all, because they just got used to the feeling of the breathing tube down their throat. On the other hand, some patients really can't tolerate being off the medication. In that case we try to wean them off quickly and extubate as soon as possible (within the hour). In almost all cases, the person is fully alert by the time we take out the breathing tube, but they can have a bit of confusion which may persist for days or even weeks after coming off sedation.
Hope this helps!
She would use a walker. Crutches and canes will unbalance you long term and cause more problems than help.
This indicates brain involvement, but most everything else sounds like peripheral nerve damage. I'm curious how an electrical injury caused non-permanent brain injury... That's the biggest issue I see. Mood changes can just be triggered by stressful events (like a major injury), so it could be that she doesn't actually have any brain damage. If an electrical current passed through her brain... those problems wouldn't just go away with therapy. They could get better, but to be honest, I hardly ever see that happen. Brain injury is HORRIBLE. As a healthcare provider it is a huge ethical dilemma for me whether I tell this to patients or not, because I don't want them to lose hope or think therapy can't help. However, personality, mood, and impulse changes are really, really hard to treat and will almost always affect someone long term. Therapy can help lessen the effects, but a lot of people with brain injuries can't even hold a job (even simple ones can be difficult, because they just can't manage time, money, or responsibilities well). Of course, some brain injuries are minor and might not affect someone long term, but... it's just really scary to me, because I see how it totally changes people's lives. They may "look" normal and everyone around them may be asking "why can't you do this simple thing that literally everyone does", but they just can't.
Speech is not in the same part of the nervous system as the arms and legs.
When writing any nerve damage (whether peripheral or central), consider where the "lesions" are. These are the areas that were hit by electricity during the initial injury.
- Central nerve damage includes the brain and spine. It is only minimally recoverable, because brain cells do not regrow, but axons do. Some areas of the brain are "plastic", meaning new axons can adapt to take over lost functions in the brain, but this is not the case in the spinal cord. If the lesion to the spinal cord is minor or incomplete (like if you have nerve compression), it can cause weakness like what you described and become better with physical therapy or surgical correction, but if it is complete, it will cause paralysis or loss of sensation or both in everything below the level of the injury. Some newer therapies focus on regrowing axons below the level of injury to take over motor functions lost by the dead cells, but they have mixed results and are not widespread.
- Peripheral nerve damage has significantly better outcomes in general. It will cause that weakness you described, but can improve significantly with physical therapy. It also can cause chronic pain. Peripheral damage refers to nerves outside the spinal cord and brain. So if electricity passed through your arm or foot, for example, you could have peripheral nerve damage to that specific location.
This makes me curious. I have talked about electrical injuries before, but just so we are all on the same page, electricity doesn't follow the pathways of the brain or nerves preferentially. The type of "electricity" that our nerves work by is very different from the type of electricity we use for power. The later is a flow of free electrons down the path of least resistance and the former is caused by the flow of sodium and potassium ions through highly regulated channels in our cell membranes. Very different and not at all related. Not saying you can't have nerve damage from electrical injuries, just saying it's not like your nervous system is receiving a "shock" when electricity passes through it. Electrical injuries are not primarily linked to nerve injuries, it's just that nerves are the tissues that won't recover as easily long term. So, your patient would have muscle, skin, and even bone or organ damage in addition to nerve damage, but these could all be recovered from within a few years. Nerve damage is just the stuff that will last.
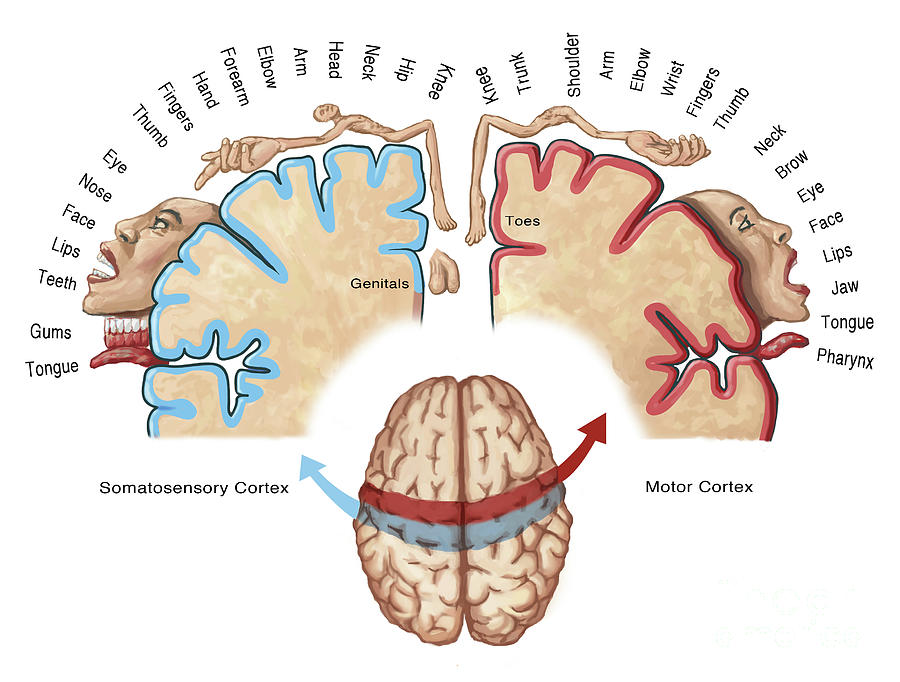
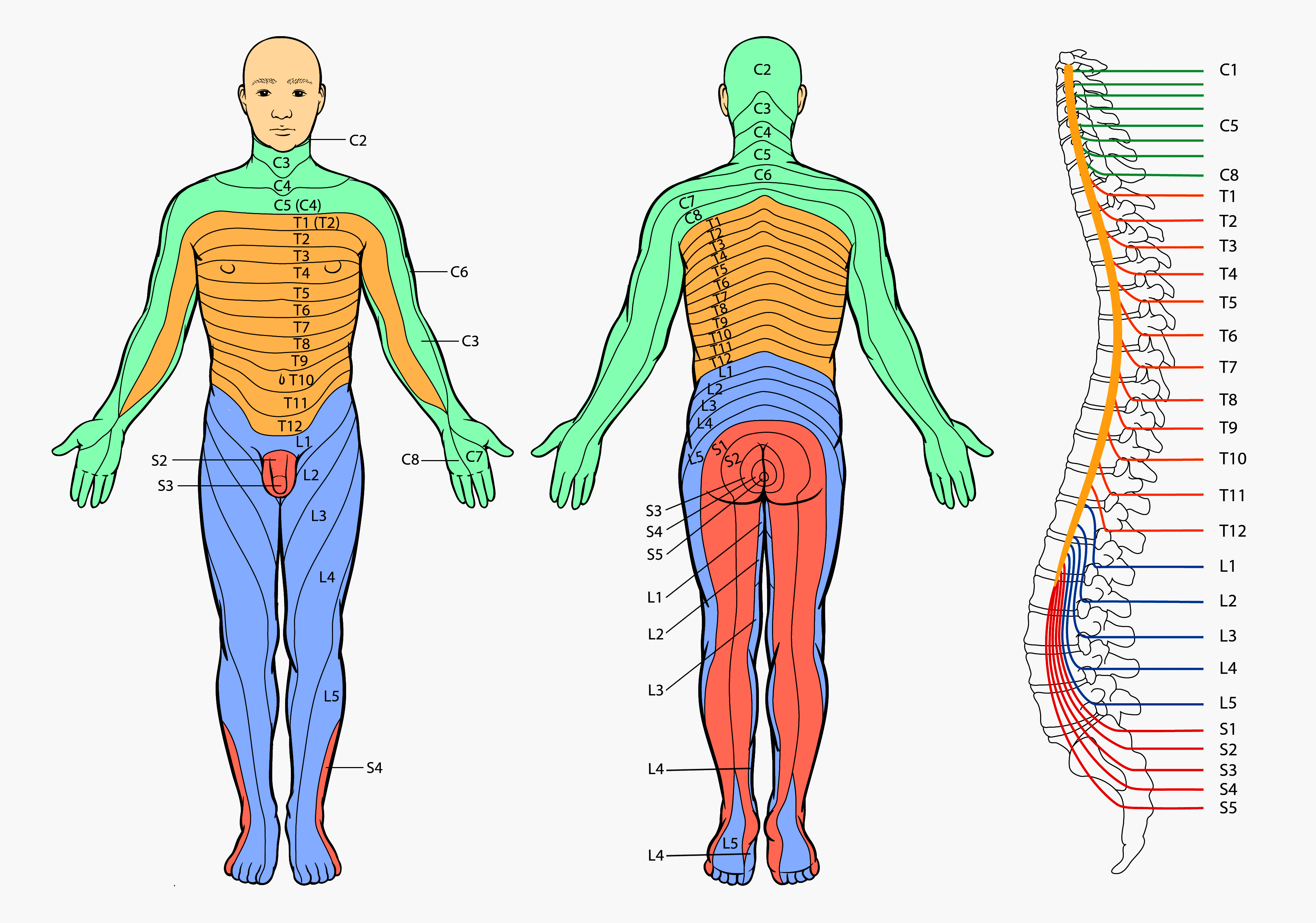
Instead, think about the path the electricity followed specifically. It doesn't really matter where, just pick and go with it. I've attached images of the homunculus of the brain (motor and sensory cortex), brain regions by function, major peripheral nerves including the cranial nerves, and the spinal cord dermatomes so you can better determine what symptoms she might have based on where the lesions are.
So, one by one:
1. Grip strength from most severe to least severe: injury to motor cortex of wrist, fingers, and thumb; injury to C7 and C8 spinal cord region; or injury to median and ulnar nerves.
2. Trouble bending over from most severe to least severe: injury to motor cortex of trunk, T1-12 spinal cord regions; or cutaneous branches on abdomen and back.
3. Balance problems again from most severe to least: cerebellum, vestibulocochlear nerve damage, all the above trunk injuries from #2, or leg injuries as described next.
4. Leg weakness: the most medial region of the motor homunculus (I honestly don't see how this could happen without significant brain injury), damage to L1-S2 nerve regions, or a whole host of peripheral nerves I won't list.
5. Speech difficulties: language center of the temporal lobe of the brain, facial cranial nerve, hypoglossal cranial nerve, glossopharyngeal cranial nerve, or trigeminal cranial nerve. Notice all of these injuries are located in the brain or very close to it. These are very high risk zones.
6. Impulse control and mood: frontal lobe of brain
I hope this helps you realize that the patient you described has very diffuse and sporadic nerve damage. I think it could happen, but I think it would be more accurate to focus on a particular area of damage rather than try to catch everything.
Hope this helps!
Gross. Good luck! Taking this info into account, as an added side note to your question about bleeding, if your character is chopping off body parts after death, those new wounds won't bleed.
1 month later

{kind=link}
{kind=link}
{kind=link}
/types-of-meniscus-tears-3862073-FINAL2-71794972dd824f7084a3fb3eb4f31a50.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:background_color(FFFFFF):format(jpeg)/images/article/en/the-12-cranial-nerves/BJlRqDAfAoB4SnDOELIzQ_Cranial_Nerves_Draft_3.png){kind=link}
{kind=link}
3 months later
Hey authors! I’m back to talk about more medical tropes that bother me, because it’s about the only thing that ever does and I can.
This time I’m giving you three tips for how to write realistic hospital scenes.
Hospitals don’t have a smell. At least we try really hard not to. We use odorless cleaners, lotions, air fresheners, and soaps. I’ve heard some authors describe hospitals as having an antiseptic smell, but even our hand sanitizers don’t have that alcohol smell that commercial brands do and bleach is very rarely used, so the only smells in hospitals come from patients and those are usually horrible. Trying to maintain odorlessness (not even clean smelling, but truly no odor) is intentional as many people are sensitive to smells.
Heart monitors don’t beep continuously with the rhythm of a patient’s heart. Like, they can, but it’s super annoying and the default settings on monitors is silence. Believe it or not, nurses actually try to minimize noise and alarms in the hospital. Sometimes it’s hard to do, but there is almost always someone around to address an alarm and silence it. Every alarm has a purpose and requires nurse attention. In fact, the only thing I hate more than alarms are patients who silence their own alarms.
 Do as I say, not as I do.
Do as I say, not as I do. 
Last, but most importantly, nurses never want to be hit on while at work. Ever. It doesn’t matter how cute the patient is, hitting on a nurse is always inappropriate and so uncomfortable. Does it happen? Yes. Absolutely. So much so that it is extremely triggering for most nurses. I’ve seen a lot of comics out there lately about nurse-patient relationships. I think this can be done alright (like in the comic Nurse’s Station), but most of the time it’s not (like in Heroic, which btw I love, but can’t stand how the propagandist is constantly flirting with his clearly uninterested nurse.) On a related note, nurses don’t hit on patients. I’ve literally never seen or heard of this. There are horror stories of medical professionals sexually assaulting patients, because, hey, it’s 2022, and there are psychos in every profession, but legitimate flirting? Nope. I have taken care of thousands of people and seen just as many boobs and penises, and I’m bisexual (so I’m not particularly picky under normal circumstances) and I have literally never been attracted to a patient nor have I heard any of my colleagues commenting on a patient’s appearance. It is one of my number one pet peeves in media when I see a group of giggling female nurses oogling over the male lead’s abs. No. Nope. No. Gross. That it so unprofessional and just wrong. It is my personal opinion that no one should objectify someone they are authority and stewardship over.
So there you have it! My thoughts on common hospital tropes! ️
Do you still review comics or novels for medical accuracy? I have one medical subplot and although not a turning point of the story, it's still kinda relevant for the characters involved. The epidemic is chickenpox and the world is reliant on magic so their medical isn't that advanced. The cure they came up with is chamomile. I'll put the link here, if you no longer do this favor, then please just disregard this comment
The topic is brought up in this chapter:
The cure is brought up in this chapter:
No need to read most of the in between chapters
Again, if you're still entertaining questions... (I came across this thread since someone bumped it, and I plan on reading everything as I go on, so I don't know yet if you already closed the questions since another person bumped it)
My character has reincarnated in a completely different world with magic and whatnot but has memories of her past life (Earth). My character remembers the reason why she died. The character is also made aware of how she reincarnated in this new world right off the bat so she was able to "process" things and calm herself, being able to remember bits and pieces of her past life (with the help of someone close to her in her past life). But she doesn't remember all of it and some of her "memories" are just things that she thinks happened, but not really. There are memories that she thinks happened, but not really. There are important/significant things that she forgot but is able to remember some insignifacant things from her past life.
Do you think it's possible or understandable that the character is experiencing/feeling this type of "jumbled" memory? Is it reasonable that she forgets her own (past life) mother only after eight years of living a new life? Or is that too short of a span of time to forget what your own mother looks like?
I absolutely am still entertaining questions! I always love to help out authors. 🥰 Give me until tonight and I’ll have a reply to both your questions up.
How many questions do you entertain per person? just curious...  <--- it's supposed to be an awkward smile....
<--- it's supposed to be an awkward smile....
Goood this is sooo helpful! thanks for this thread!
Do you have any info on Port-wine stain (aka nevus flammeus)?
I have a character who was born with fair skin but developed reddish-purple patches on his skin as he got older. I am not sure if I should label my character as having port-wine stain or just make up a fake condition that is similar to it (my comic is a fantasy).
Sure! This is an easy one.
Nevus Flammeus is a congenital condition, so your character would be born with it. It does not develop as you age, but can become more prominent or expand with age.
However, there are other conditions which can cause red, purple, and brown patches. Where those spots appear, what they look like, how large they are, and what color they are will determine what they are called.
Granuloma annulare is probably the closest thing I can find to portwine stains that occurs in adulthood. They are commonly found on the ankles or hands and are painless, red/purple patches that develop over time, typically in adults.
Other Painless Spots:
Liver spots are common on the arms and abdomen while melasma are found on the face. Both are painless, benign (meaning not life threatening) conditions. Purpura can cause purple-red spots and are common in old age. In younger characters (under 65) it could be an indication of an underlying bleeding disorder. Scleroderma are very small purple-red spots that sometimes look like an exploding starburst. Morphea are light brown, sometimes large spots that can cover the face, neck, and torso. Keloids are purple-red raised scar tissue that can expand from an injury to cover a ton of body surface area. So if your character was cut by a blade or knife he might have keloid formation over those spots, extending into massive purple-red lesions. Spider angioma can be small purple spots which look like spiderwebs.
Everything else which is not infectious related will be itchy or painful.
Annoying/Itchy Chronic Discoloration Lesions:
Nummular eczema causes red, sometimes purple patches on the skin, but are extremely itchy and lesions will move over time. Uritcaria pigmentosa lesions are sometimes brownish red, but this is more commonly found in children and usually clears by adulthood (although it can stick around). Psoriasis causes purple-red elevated plaques of dry skin (often flaky and white) commonly over the knees and elbows, but can happen anywhere (although generally not the face) and are extremely uncomfortable (but is a chronic condition that people just live with and often don't get treated ever).
Let me know if any of these conditions peak your interest and you would like any more information!